
Bacteria
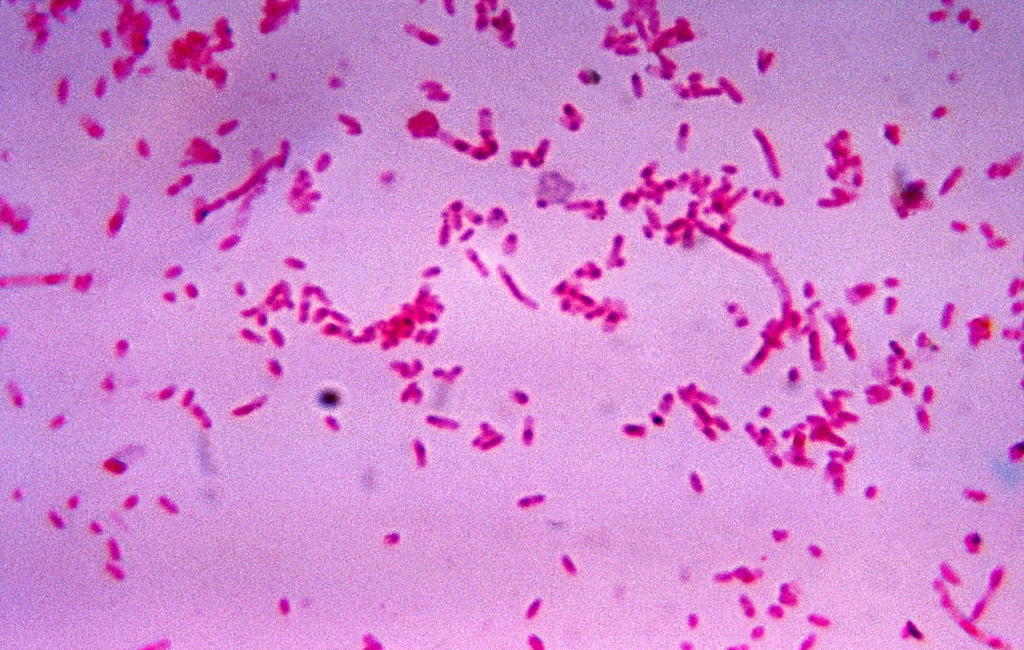
Fusobacterium necrophorum is a Gram-negative, non-motile, non-spore-forming anaerobic pleomorphic bacterium. It may appear in coccobacillus or filamentous forms, which are more common in younger cultures.
It is a member of the normal bacterial flora of the oropharynx, genitourinary tract, and gastrointestinal tract.
Culture and identification
There are 14 species of Fusobacterium, 10 of which are identified from humans. The most commonly isolated species are F necrophorum and F nucleatum. F nucleatum is a spindle-shaped gram-negative rod.
F necrophorum is –
- Gram-negative but often stained irregularly.
- Pleomorphic – coccobacillary or filamentous forms. Filamentous forms are more common in young culture.
- 1-3mm, beta-haemolytic, translucent to granular and opaque colonies
- Indole positive and fluoresce under UV light and produce lipase on egg yolk agar
- Aesculin negative, catalase negative
Identification can be made by API 20A, API rapid ID 32A or MALDI ToF
Pathogenicity:
- Toxin – leukotoxin
- Activation of plasminogen, platelet aggregation, and production of haemagglutinin
- Binding to the factor H, a complement controlling glycoprotein
Clinical features
Pharyngitis
Especially in adolescents and adults – up to 20% of cases. The signs/symptoms are indistinguishable from Group A Streptococcus pharyngitis. Fever, exudative tonsillitis, and cervical adenopathy, but the cough is absent in most cases.
Peritonsillar abscess
A complication of pharyngitis. F necrophorum is one of the commonest causes.
Lemierre syndrome (postanginal sepsis)
septic thrombophlebitis of the internal jugular vein. 80% of Lemierre syndrome is due to F necrophorum. It usually follows pharyngitis – the patient presents with neck pain, swelling, signs of sepsis and persistent pharyngitis symptoms. Complications – septic shock, metastatic complication (septic emboli and abscess to lungs, joints, liver, peritoneum, kidneys, and brain). Diagnosis – CT with contrast, MRI, and blood culture.
Middle ear infection, mastoiditis
Endocarditis
It is a rare cause of endocarditis.
Treatment
F necrophorum is usually susceptible to penicillin. However, some strains produce beta-lactamase. So in some cases, treatment failure may occur with penicillin/amoxicillin.
Antibiotics that can be used to treat F necrophorum infection
- Coamoxiclav, pip-tazobactam
- Clindamycin
- Carbapenems
- Metronidazole
Lemierre’s syndrome – may need combination therapy, debridement, incision-drainage