
An emerging pathogen
- Actinotignum schaalii is a novel/emerging uropathogen.
- It was first discovered in 1997, but it was called Actinobaculum schaalii. In 2015, the genus Actinobaculum was divided into two genera Actinotignum, which contains Actinotignum schaalii and Actinobaculum, including Actinobaculum suis.
- It is a commensal organism of the human urinary tract, female genital tract and skin, especially the groin area.
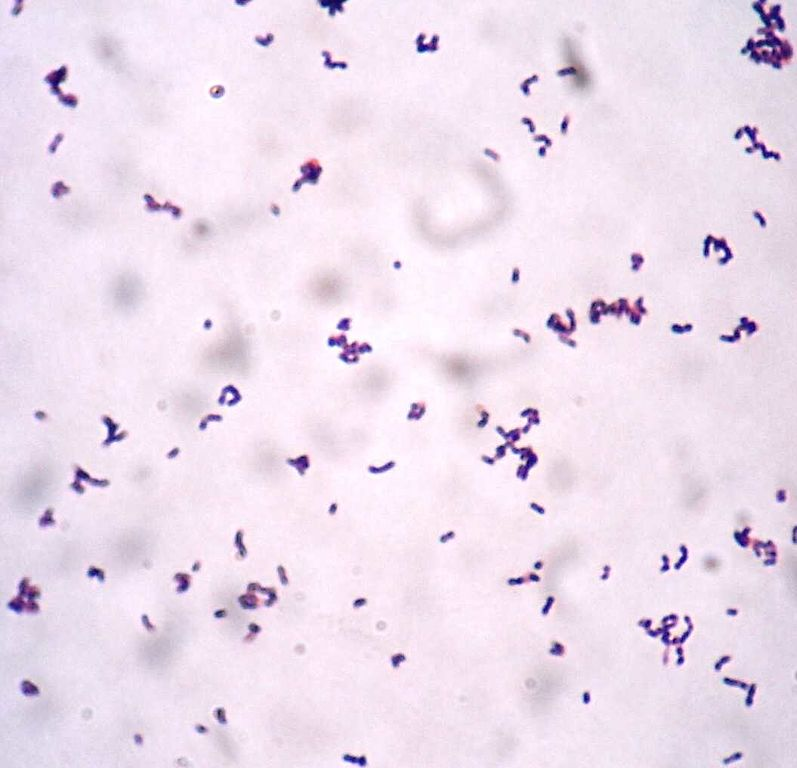
Actinotignum schaalii gram stain (pic Manurx27, Wikipedia)
What infection does it cause, and who is mostly affected?

- Actinotignum schaalii is most commonly associated with urinary tract infections, especially in older people. However, cases from children have been reported as well.
- Actinotignum UTI is usually associated with immunosuppression and urological abnormalities like bladder cancer, prostate cancer, neurological bladder, benign hypertrophy of the prostate, urethral stricture, catheterization, etcetera.
- Other infections reported in the literature are bacteraemia, abscess, Fournier’s gangrene, endocarditis, cellulitis and discitis.
How to identify Actinotignum schaalii in the lab?
- It is a thin Gram-positive rod, often slightly curved.
- It is a facultative anaerobe.
- It produces non-haemolytic or weakly alpha haemolytic colonies on the blood agar.
- It is also a slow-growing organism.
- Most laboratories in the UK culture the urine on a chromogenic agar and incubate it for 24 hours only. This may result in failure to grow this bacteria.
- This bacteria is CAMP, catalase, and oxidase negative.
- It is also negative for nitrate reduction. So it will not give a nitrate-positive reaction on the dipstick test when it causes UTI.
- It can be identified using 16S rRNA and MALDI ToF technology.
- Commercial systems are known to misidentify it as Gardnerella, Arcanobacterium or Actinomyces.
How do we treat infection caused by Actinotignum schaalii infection?
- There is no guideline for treatment; hence specialist opinion should be taken as it is crucial to consider pharmacokinetics and the pharmacodynamics of the antibiotics depending on the site of infection.
- It has been reported that it is susceptible to beta-lactam antibiotics, except for mecillinam.
- It is also susceptible to doxycycline, vancomycin, teicoplanin, linezolid, rifampicin, nitrofurantoin, gentamicin and 3rd and 4th generation quinolones like levofloxacin and moxifloxacin.
- 2nd generation quinolones like ciprofloxacin should not be used as it is mostly resistant. Another antibiotic to which this bacteria is consistently resistant is cotrimoxazole.
- Variable resistance had been reported to mecillinam, Fosfomycin, macrolides and clindamycin.
Actinotignum schaalii presentation.
(Youtube)